Self Pay Agreement Form
Self Pay Agreement Form - Private pay agreement name of patient: This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services. _____ at medpsych health services, our dedicated team is fully committed to ensuring. Service self pay agreement form. Self pay agreement form patient name: _____ i, _____ (print name of person responsible. I am not covered under a health insurance plan and/or. Self pay no insurance waiver: _____ if applicable, name of parent/legal guardian:
_____ i, _____ (print name of person responsible. Self pay no insurance waiver: Self pay agreement form patient name: I am not covered under a health insurance plan and/or. Private pay agreement name of patient: Service self pay agreement form. _____ at medpsych health services, our dedicated team is fully committed to ensuring. _____ if applicable, name of parent/legal guardian: This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services.
Self pay no insurance waiver: _____ at medpsych health services, our dedicated team is fully committed to ensuring. Private pay agreement name of patient: This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services. Self pay agreement form patient name: _____ i, _____ (print name of person responsible. I am not covered under a health insurance plan and/or. Service self pay agreement form. _____ if applicable, name of parent/legal guardian:
Payment Agreement 41 Templates & Contracts ᐅ TemplateLab
I am not covered under a health insurance plan and/or. Self pay no insurance waiver: _____ if applicable, name of parent/legal guardian: _____ i, _____ (print name of person responsible. Service self pay agreement form.
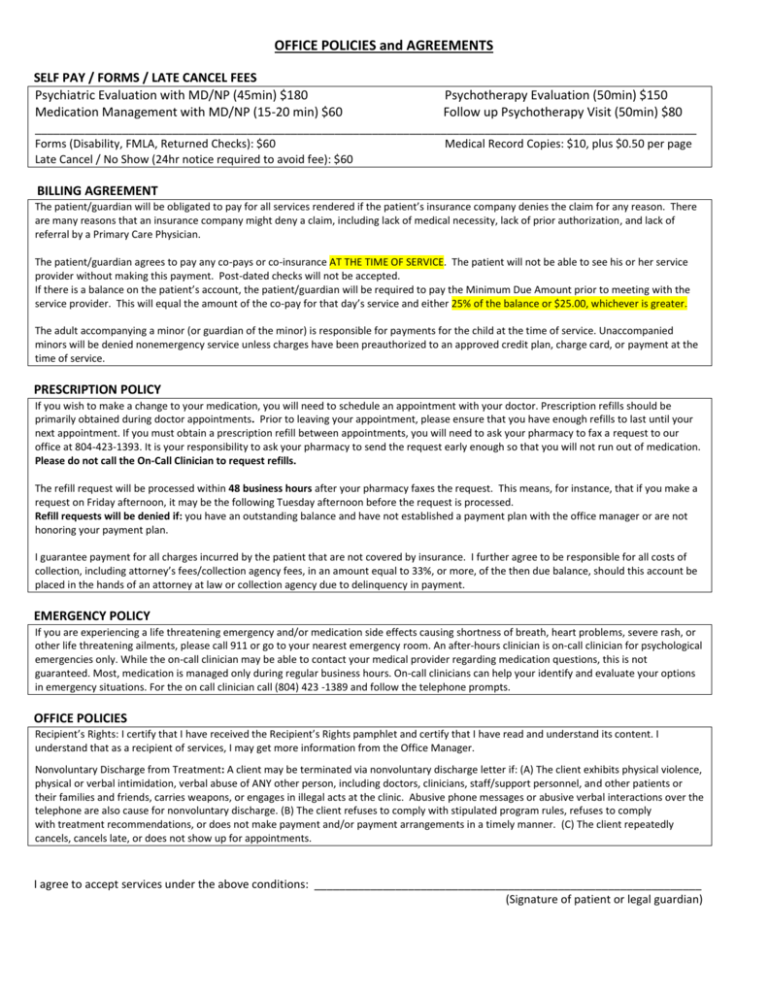
OFFICE POLICIES and AGREEMENTS SELF PAY / FORMS / LATE
Private pay agreement name of patient: Service self pay agreement form. _____ i, _____ (print name of person responsible. Self pay no insurance waiver: This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services.
Fillable Online SelfPay Agreement. Selfpay agreement for member Fax
_____ if applicable, name of parent/legal guardian: _____ at medpsych health services, our dedicated team is fully committed to ensuring. Service self pay agreement form. Self pay no insurance waiver: Private pay agreement name of patient:
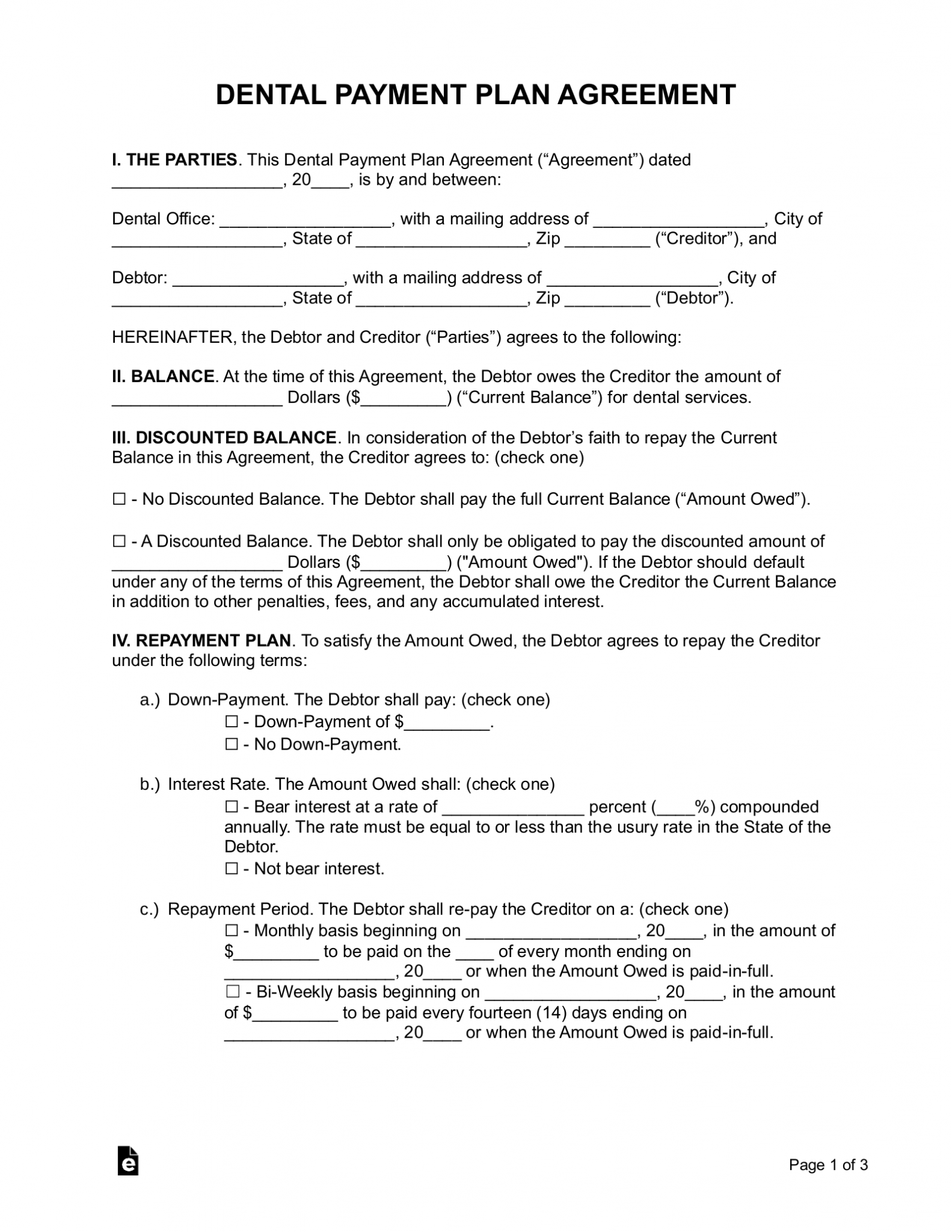
Free Dental Payment Plan Agreement PDF Word eForms
_____ at medpsych health services, our dedicated team is fully committed to ensuring. Self pay agreement form patient name: Service self pay agreement form. Self pay no insurance waiver: I am not covered under a health insurance plan and/or.

Dental Payment Plan Agreement Template Printable Payment agreement
Self pay agreement form patient name: I am not covered under a health insurance plan and/or. This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services. Self pay no insurance waiver: Service self pay agreement form.
Fillable Online Patient payment agreement healthcare templates.office
Private pay agreement name of patient: Self pay agreement form patient name: _____ if applicable, name of parent/legal guardian: Self pay no insurance waiver: _____ i, _____ (print name of person responsible.

Dental Payment Plan Agreement Template Lovely Agreement Template
Self pay no insurance waiver: Self pay agreement form patient name: _____ i, _____ (print name of person responsible. This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services. I am not covered under a health insurance plan and/or.

Simple Payment Agreement Template Lovely 4 Medical Payment Plan
I am not covered under a health insurance plan and/or. Service self pay agreement form. _____ i, _____ (print name of person responsible. This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services. _____ at medpsych health services, our dedicated team is fully committed to ensuring.
Free Payment Plan Agreement Template PDF Word eForms
Private pay agreement name of patient: Service self pay agreement form. _____ i, _____ (print name of person responsible. _____ if applicable, name of parent/legal guardian: I am not covered under a health insurance plan and/or.
Wage Agreement Template
Private pay agreement name of patient: _____ if applicable, name of parent/legal guardian: _____ at medpsych health services, our dedicated team is fully committed to ensuring. Self pay no insurance waiver: This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services.
I Am Not Covered Under A Health Insurance Plan And/Or.
Private pay agreement name of patient: _____ at medpsych health services, our dedicated team is fully committed to ensuring. Service self pay agreement form. _____ if applicable, name of parent/legal guardian:
_____ I, _____ (Print Name Of Person Responsible.
Self pay agreement form patient name: Self pay no insurance waiver: This form is for patients who register as private pay and pay by cash, check, or debit/credit card for psychiatry services.