Printable Blank Medical History Form
Printable Blank Medical History Form - We design printable medical history forms to make it simple for patients and healthcare providers. Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history:
Feel free to ask your primary care physician for assistance. We design printable medical history forms to make it simple for patients and healthcare providers. Please complete this form to provide information regarding your medical condition. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history:
Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Feel free to ask your primary care physician for assistance. We design printable medical history forms to make it simple for patients and healthcare providers. Please complete this form to provide information regarding your medical condition.

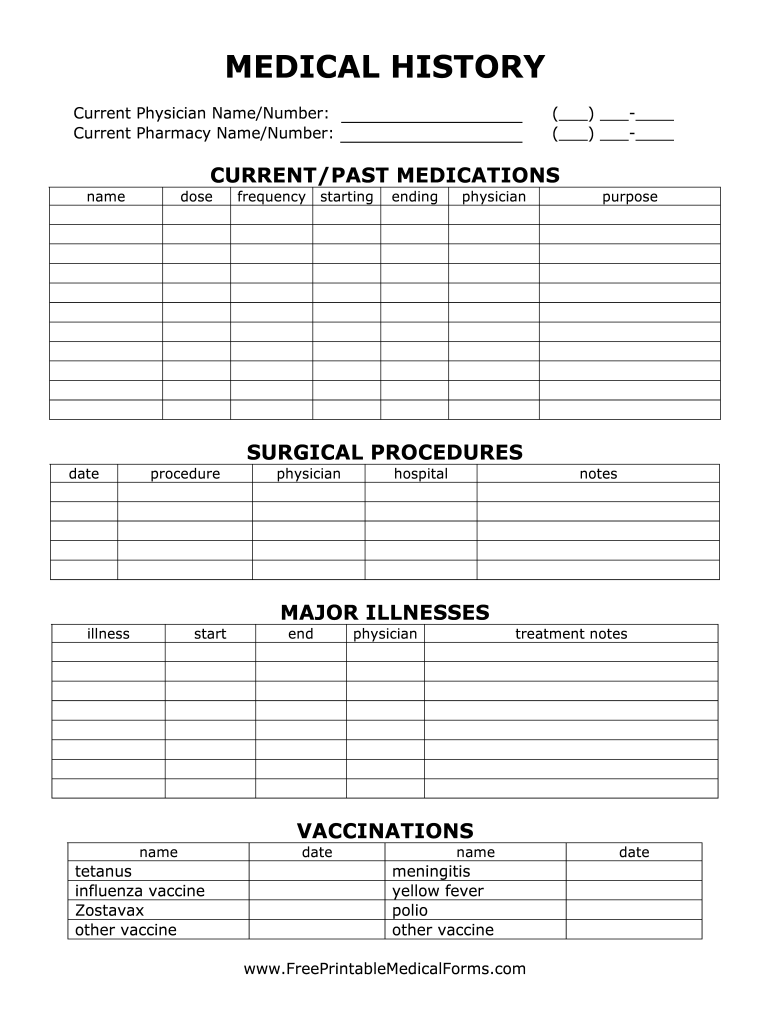
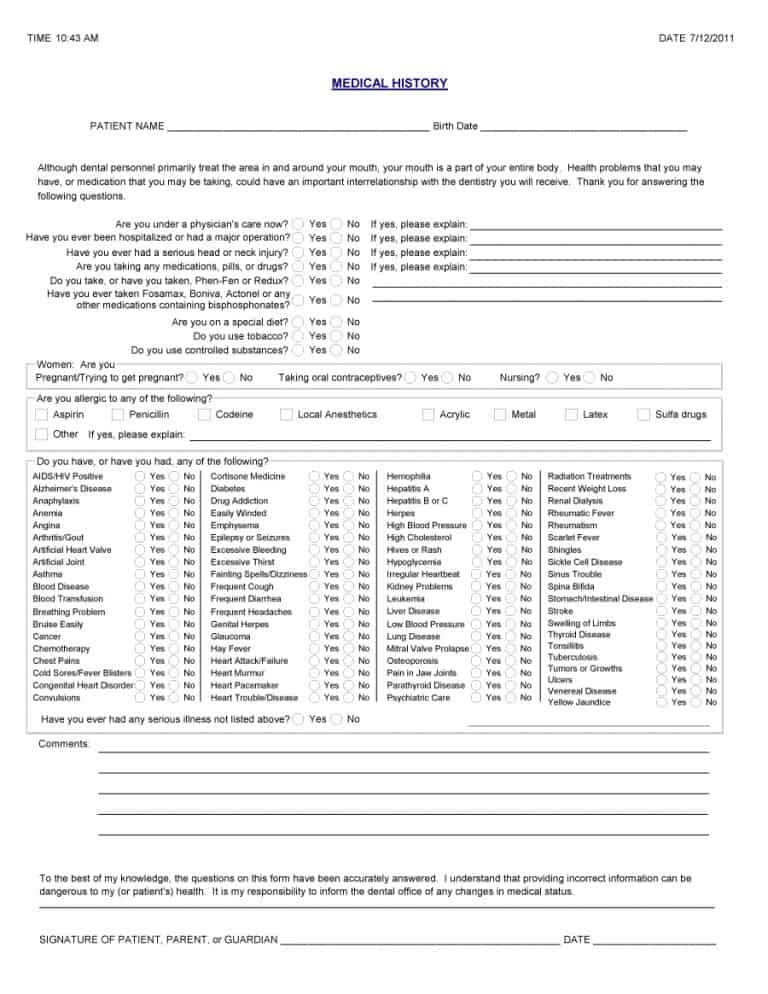
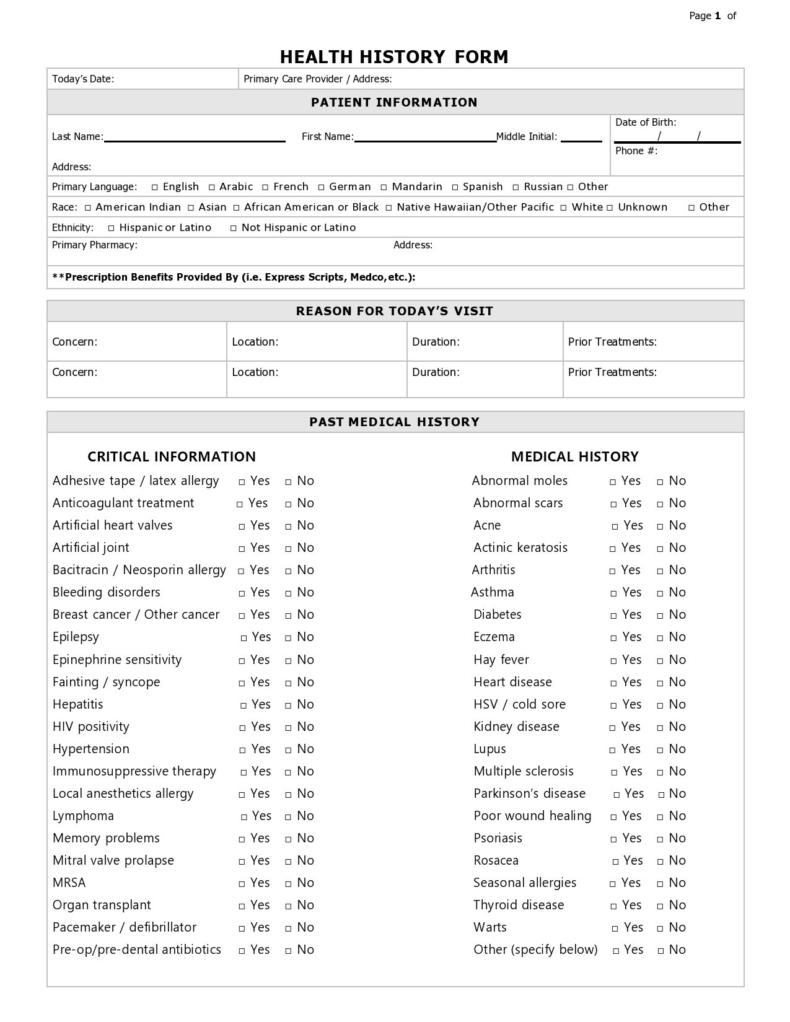
the medical history worksheet is shown in this file, and contains
Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Feel free to ask your primary care physician for assistance. We design printable medical history forms to make it simple for patients and healthcare providers. Please complete this form to provide information regarding your medical condition.
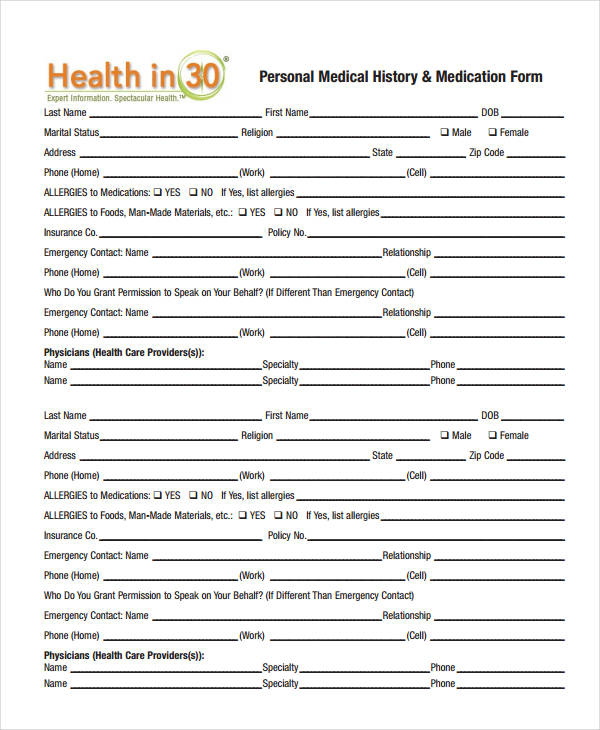
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-37.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
We design printable medical history forms to make it simple for patients and healthcare providers. Feel free to ask your primary care physician for assistance. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition.

Medical History Form Download the free Printable Basic Blank Medical
We design printable medical history forms to make it simple for patients and healthcare providers. Feel free to ask your primary care physician for assistance. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition.
Printable Blank Medical History Form Printable Templates
We design printable medical history forms to make it simple for patients and healthcare providers. Feel free to ask your primary care physician for assistance. Please complete this form to provide information regarding your medical condition. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history:
Medical History Form Printable templates free printable
Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance. We design printable medical history forms to make it simple for patients and healthcare providers.

Printable Blank Medical History Form Printable Word Searches
Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition. We design printable medical history forms to make it simple for patients and healthcare providers. Feel free to ask your primary care physician for assistance.
Blank Medical History Form Printable Printable Forms Free Online
Feel free to ask your primary care physician for assistance. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition. We design printable medical history forms to make it simple for patients and healthcare providers.
Medical History Forms 10 Free PDF Printables Printablee
Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition. Feel free to ask your primary care physician for assistance. We design printable medical history forms to make it simple for patients and healthcare providers.
Printable Blank Medical History Form Fillable Form 2023
Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Feel free to ask your primary care physician for assistance. We design printable medical history forms to make it simple for patients and healthcare providers. Please complete this form to provide information regarding your medical condition.
Printable Medical History Form
Please complete this form to provide information regarding your medical condition. We design printable medical history forms to make it simple for patients and healthcare providers. Feel free to ask your primary care physician for assistance. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history:
Feel Free To Ask Your Primary Care Physician For Assistance.
We design printable medical history forms to make it simple for patients and healthcare providers. Medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Please complete this form to provide information regarding your medical condition.