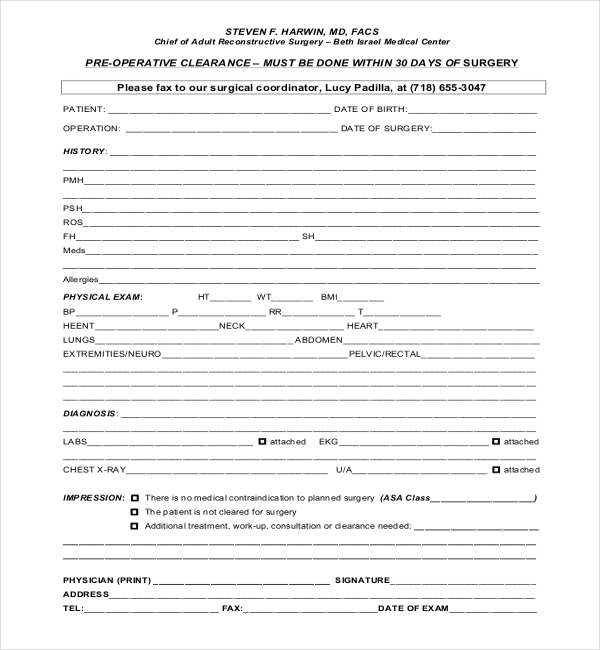
Preoperative Clearance Form
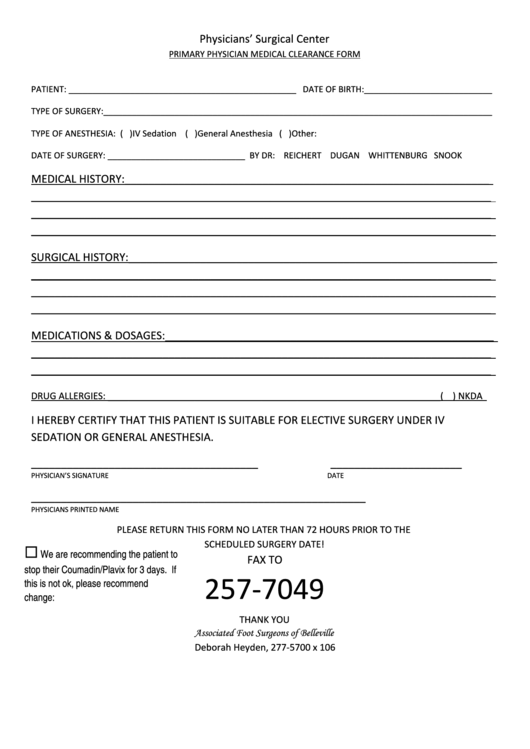
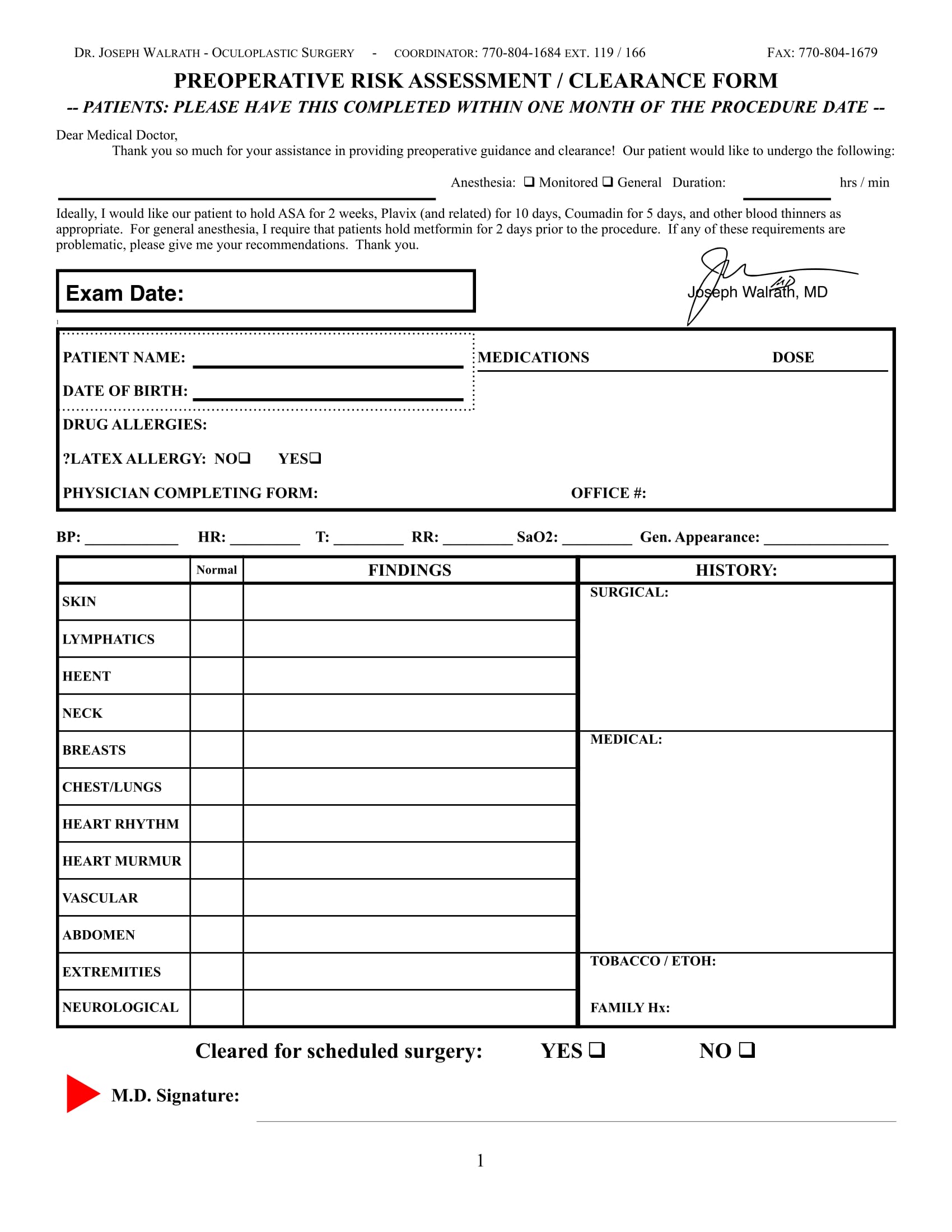
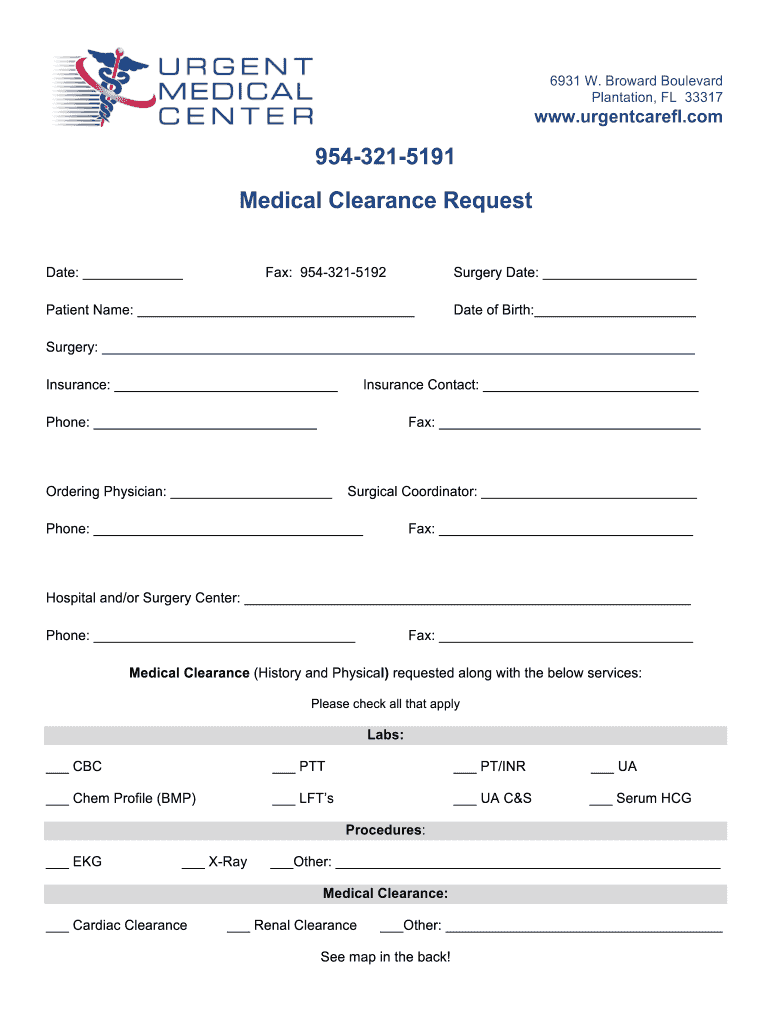
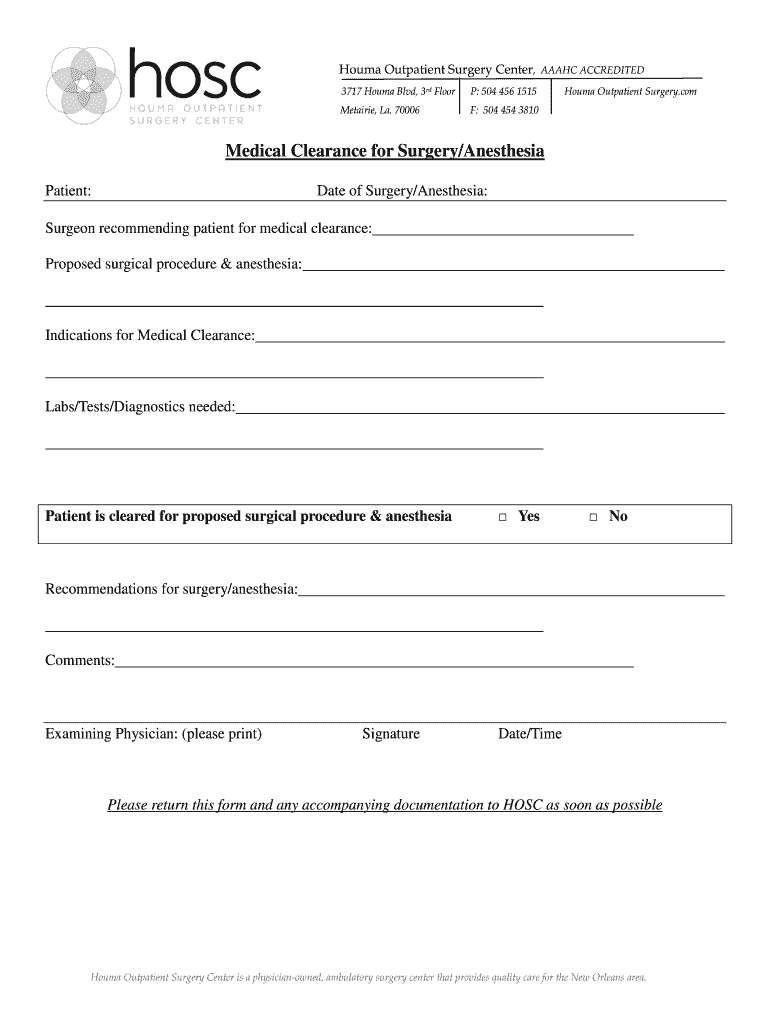
Preoperative Clearance Form - We are requesting a medical evaluation for surgical clearance. We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: Evaluation must be completed within 30 days of the surgery.
Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance.
The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance. We are requesting a medical evaluation for surgical clearance. Evaluation must be completed within 30 days of the surgery.
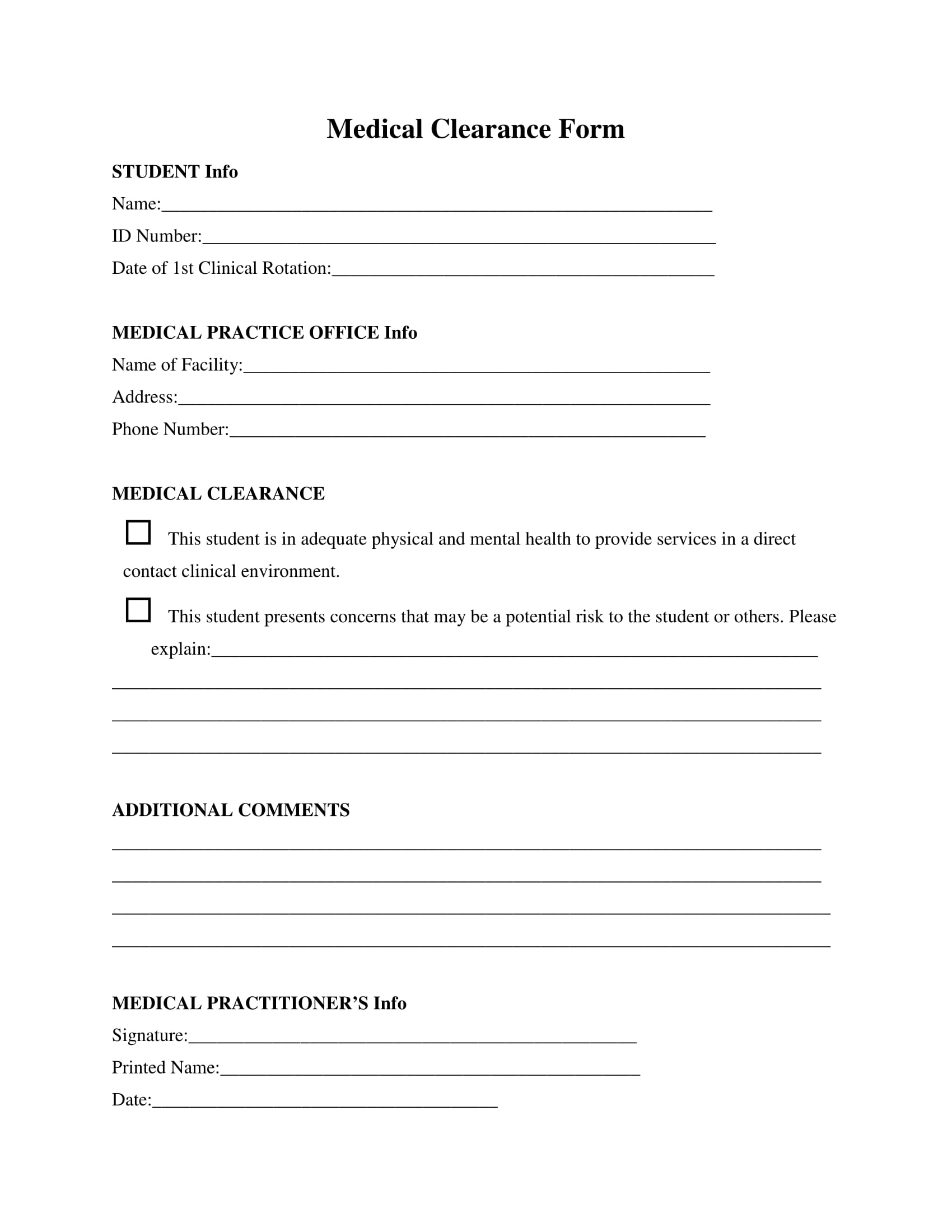
FREE 30+ Medical Clearance Form Samples in PDF MS Word
Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance.
Surgical Medical Clearance Form
We are requesting a medical evaluation for surgical clearance. Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure:
FREE 29+ Sample Medical Clearance Forms in PDF Word Excel
The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance. Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance.
Free 30 Sample Medical Clearance Forms In Pdf Ms Word
We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance. Evaluation must be completed within 30 days of the surgery.
Printable Dental Clearance Form
The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance. We are requesting a medical evaluation for surgical clearance. Evaluation must be completed within 30 days of the surgery.
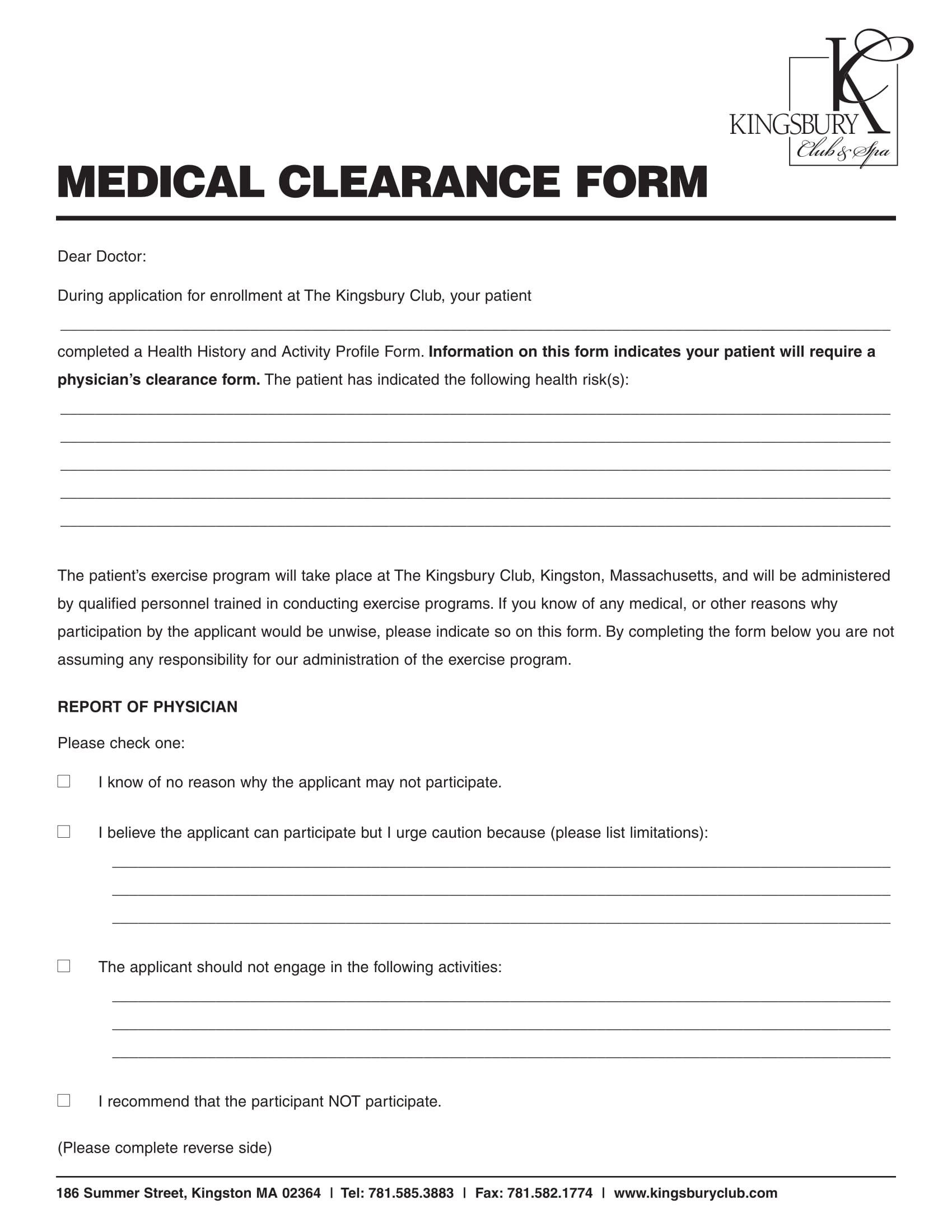
FREE 31+ Medical Clearance Forms in PDF MS Word
Evaluation must be completed within 30 days of the surgery. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance. We are requesting a medical evaluation for surgical clearance.
Printable Medical Clearance Form Complete with ease airSlate SignNow
We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance.
Medical Clearance Form Fill Online, Printable, Fillable, Blank
Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance.
Printable Medical Clearance Form For Surgery Printable Word Searches
The following test(s) are to be obtained prior to the planned surgical procedure: Evaluation must be completed within 30 days of the surgery. We are requesting a medical evaluation for surgical clearance. We are requesting a medical evaluation for surgical clearance.
FREE 31+ Medical Clearance Forms in PDF MS Word
We are requesting a medical evaluation for surgical clearance. Evaluation must be completed within 30 days of the surgery. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance.
Evaluation Must Be Completed Within 30 Days Of The Surgery.
We are requesting a medical evaluation for surgical clearance. The following test(s) are to be obtained prior to the planned surgical procedure: We are requesting a medical evaluation for surgical clearance.