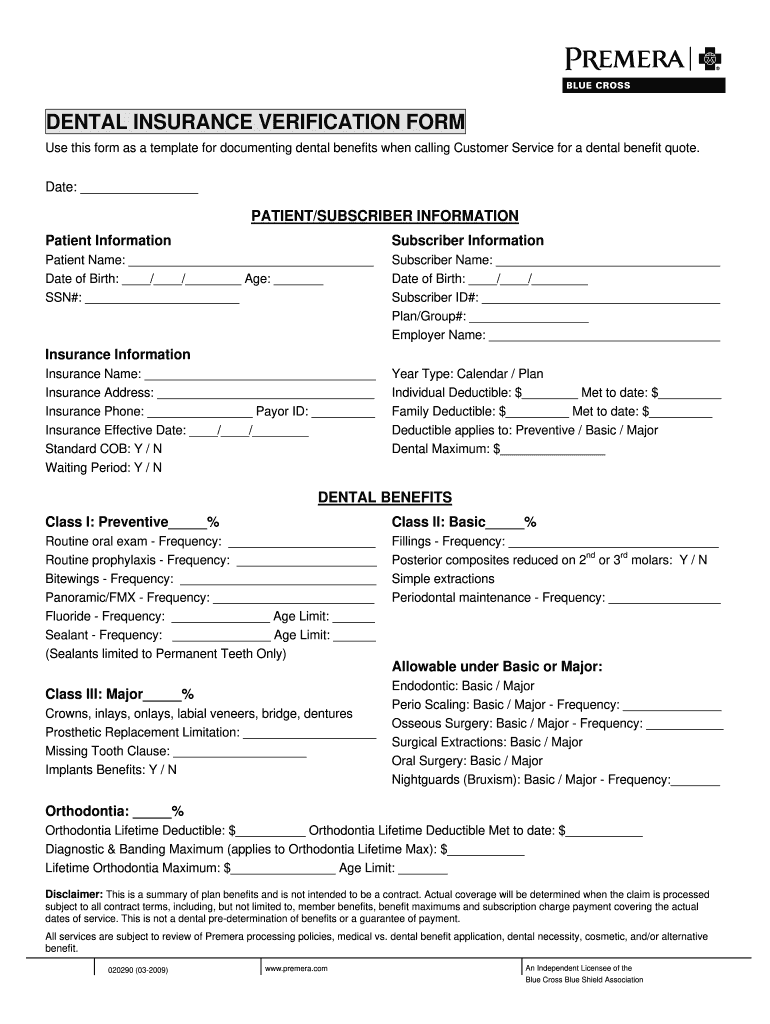
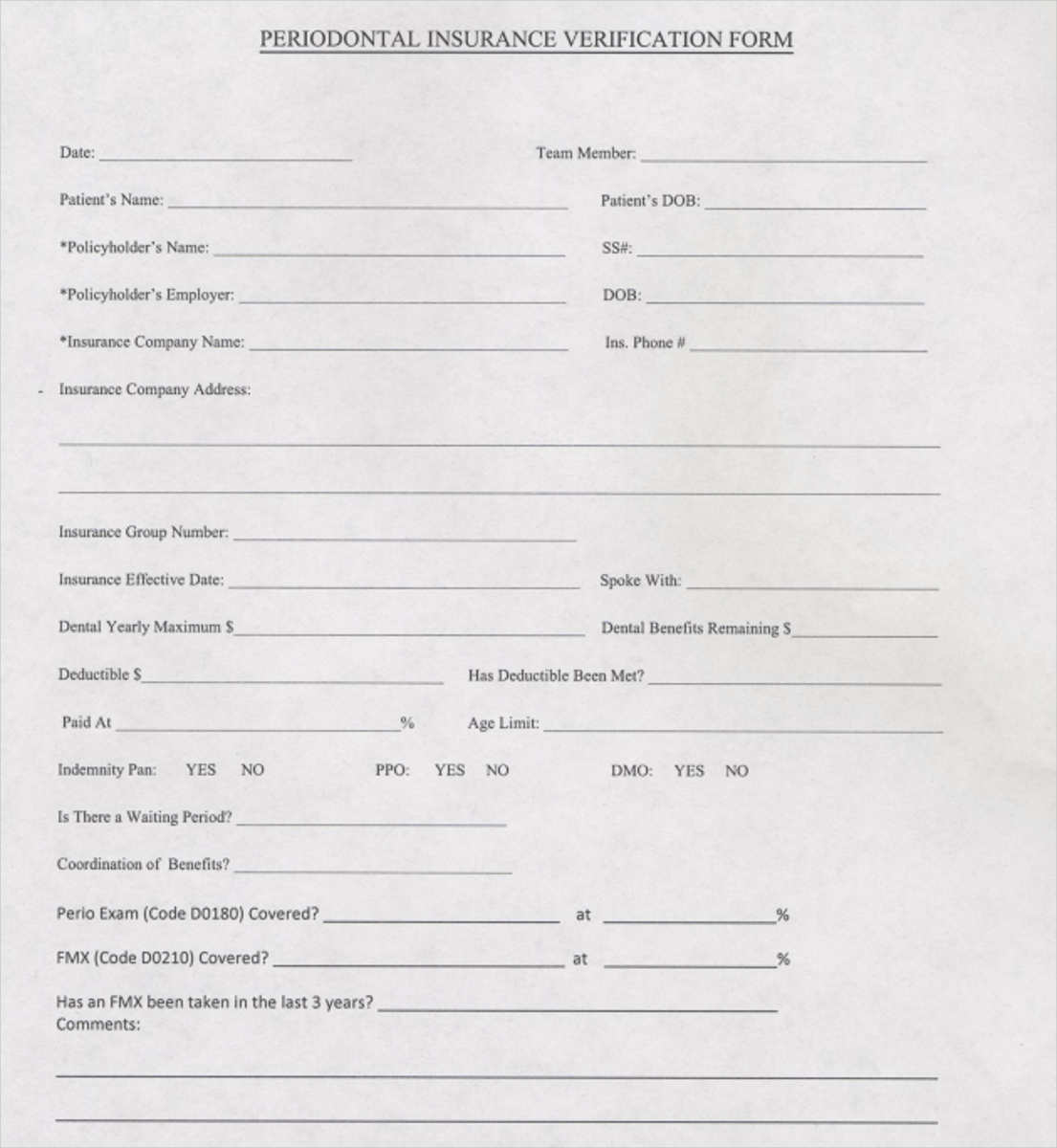
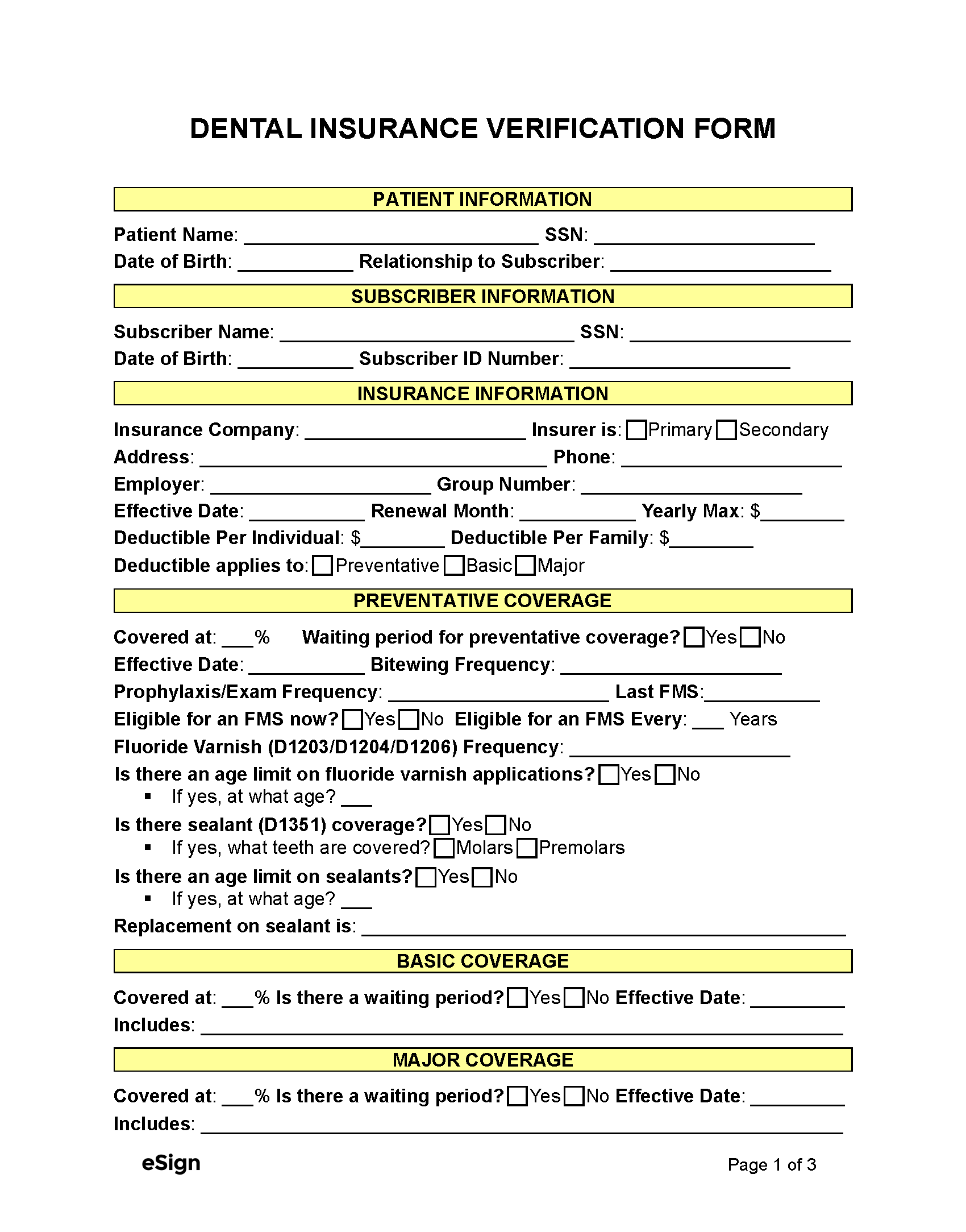
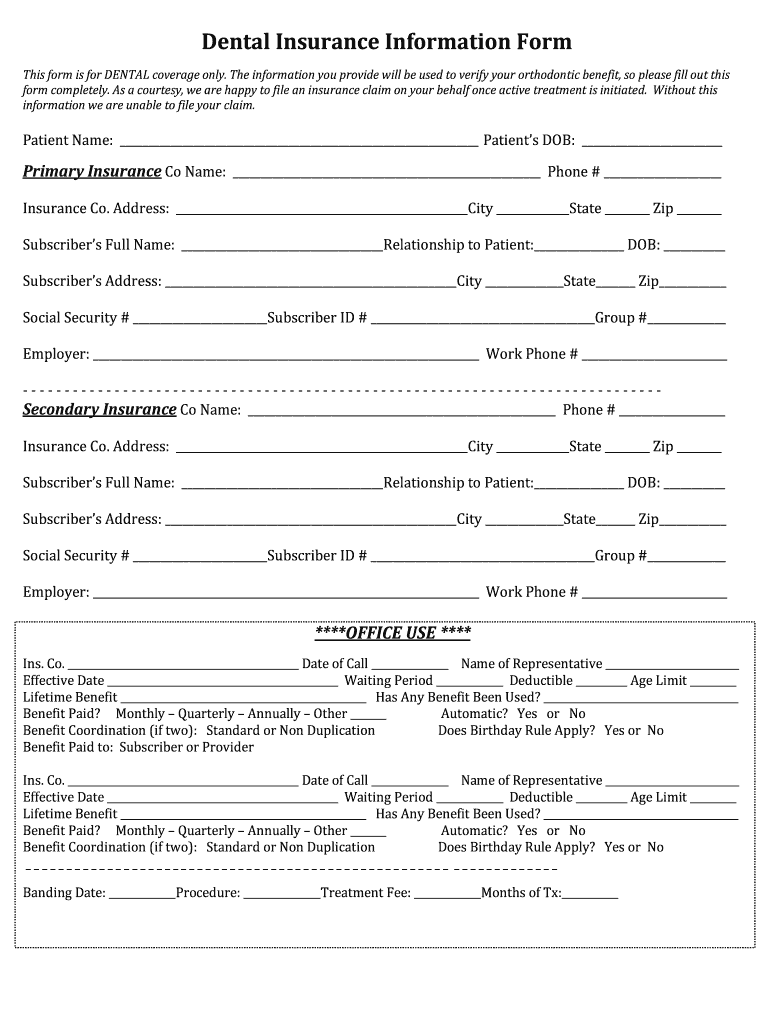
Insurance Breakdown Form
Insurance Breakdown Form - Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)? Yes no if yes, when?
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)?

Template Dental Insurance Breakdown Form INSURANCE DAY
Insurance information does the patient have any history of srp (d4341/d4342)? Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____
Dental Insurance Breakdown 20092024 Form Fill Out and Sign Printable
Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)?

Insurance Form Templates for Online Use 123 Form Builder
Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?

Template Dental Insurance Breakdown Form
Insurance information does the patient have any history of srp (d4341/d4342)? Yes no if yes, when? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____

Dental Insurance Verification Form — The Superbill Blog
Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?

Template Dental Insurance Breakdown Form
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Insurance information does the patient have any history of srp (d4341/d4342)? Yes no if yes, when?
best dental insurance
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)?
Free Dental Insurance Verification Form PDF Word
Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when? Insurance information does the patient have any history of srp (d4341/d4342)?
Dental Insurance Information Form Fill Online, Printable, Fillable
Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?

5 Tips Reviewing a Patient's Dental Insurance Breakdown Forms
Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____ Yes no if yes, when?
Yes No If Yes, When?
Insurance information does the patient have any history of srp (d4341/d4342)? Insurance breakdown form date _____ patient/subscriber information patient information patient name_____ date of birth_____